
Health Costs Are Becoming a Wealthspan Risk
New AARP and KFF findings show that many older adults are not just worried about retirement in the abstract. Rising everyday costs and Medicare out-of-pocket expenses are squeezing the money people rely on to stay independent.
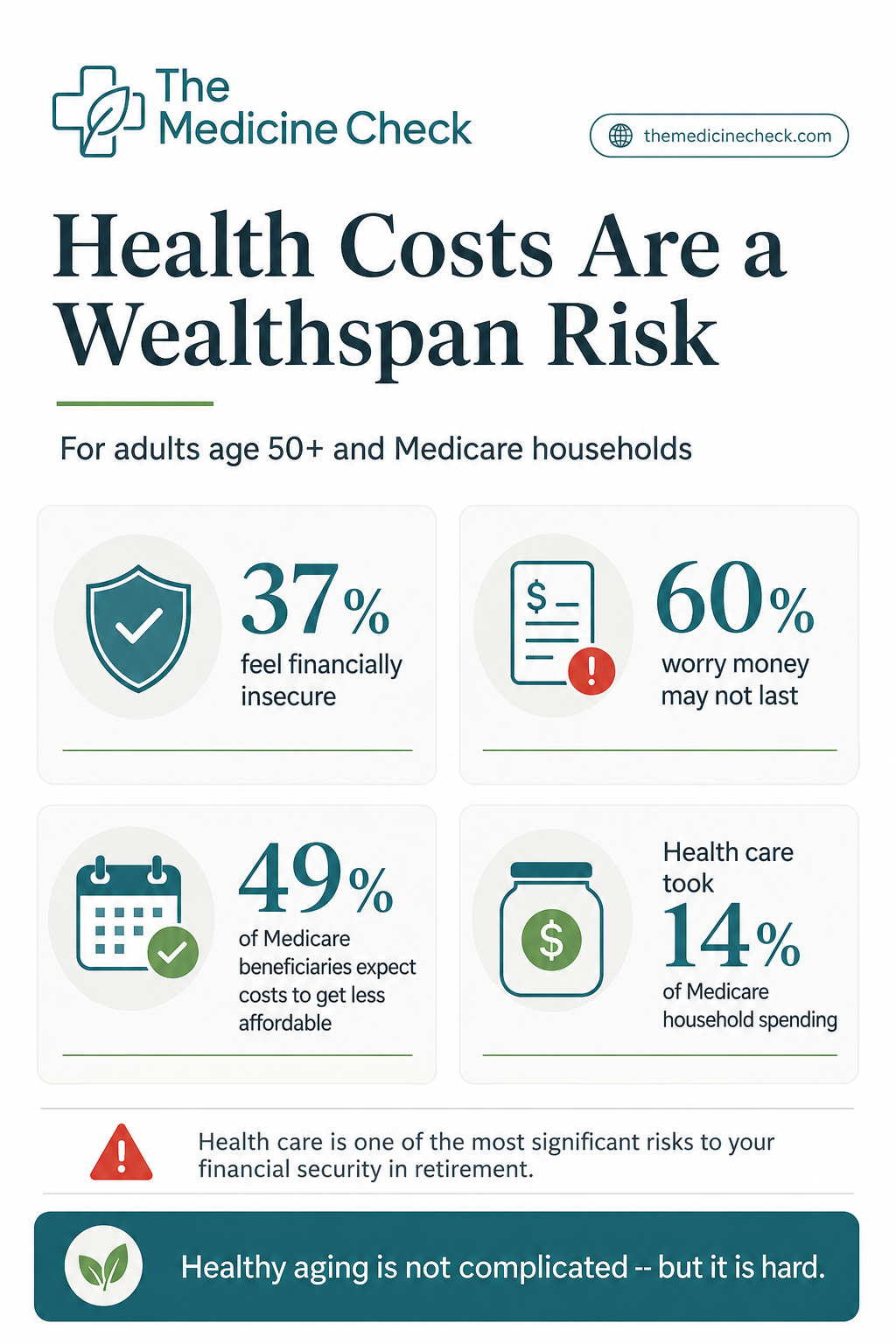
Infographic summarizing health-care affordability as a Wealthspan risk, with callouts from AARP and KFF on financial insecurity, retirement worry, Medicare affordability expectations, and health-care spending in Medicare households.
The Wealthspan question hiding inside health-care inflation
Health-care costs are often treated as a retirement footnote: a line item to estimate after housing, food, travel, and taxes. This week’s data argue for a different framing. Health-care affordability is a Wealthspan issue because it can affect how long savings last, whether people delay care, and how much freedom they have to make healthy choices as they age.
On May 28, 2026, AARP released its 2026 Financial Security Trends Survey, based on a January survey of 6,736 adults age 30 and older. Among adults 50 and older, AARP reported that 37% feel financially insecure, 60% worry about having enough money to last through retirement, and 42% of those not yet retired have less than $50,000 in retirement savings. AARP also found that 52% of older adults say their health-care costs are higher than they were 12 months ago.
The day before, KFF published a Medicare affordability brief showing why this matters even after age 65. Medicare is essential coverage for about 70 million people, but it does not erase premiums, cost sharing, drug costs, dental and vision gaps, or long-term care exposure. KFF reported that 49% of Medicare beneficiaries age 65 and older expect their health-care costs to become less affordable in the next year.
Why this is bigger than one monthly bill
The key Wealthspan lesson is that medical costs are not just unpredictable emergencies. They are also recurring expenses that compete with groceries, housing, transportation, debt payments, and retirement savings.
KFF estimated that in 2023 Medicare beneficiaries spent an average of $6,459 out of pocket on health care, including premiums and health services. In 2024, health care accounted for 14% of total household spending for Medicare households, compared with 6% for non-Medicare households. KFF also noted that one in four Medicare beneficiaries had income below $24,600 per person in 2024, and one in four had savings below $18,950 per person.
That combination is the pressure point: modest income, modest savings, and a health-care system where coverage still leaves meaningful bills. For a healthy-aging audience, this is not only about dollars. Cost pressure can shape whether people fill prescriptions, attend follow-up appointments, choose safer housing, hire help after an injury, or preserve savings for later-life care.
The evidence is strong enough to act on, but not to panic over
The AARP findings are survey data, so they tell us how people report their financial situation and worries. They do not prove that rising costs caused every change in security or savings. But the survey is large, nationally oriented, and directly relevant to adults approaching or living in retirement.
KFF’s Medicare brief is not a clinical trial or a personal planning model. It is a policy and data synthesis, drawing from multiple sources to show the affordability burden among Medicare beneficiaries. Its main message is consistent with other retirement-health-cost analyses: Medicare is a foundation, not a complete financial shield.
EBRI’s 2026 retirement health-cost report adds a planning benchmark. It estimated that a 65-year-old man enrolled in Medigap with average premiums would need $212,000 in savings to have a 90% chance of covering retirement health expenses, while a 65-year-old woman would need $252,000. For a couple enrolled in Medigap with average premiums, the 90% target was $405,000. These estimates do not include every possible long-term care cost, and actual needs vary widely, but they make the scale of the issue harder to ignore.
What this means for your Wealthspan plan
The practical takeaway is not to guess one giant number and feel defeated. A stronger approach is to build health-care costs into an annual review, the same way you might review investments, insurance, taxes, debt, and emergency savings.
First, separate routine costs from shock costs. Routine costs include premiums, expected copays, prescriptions, dental and vision care, and regular visits. Shock costs include a hospitalization, a new diagnosis, an expensive drug, a caregiving need, or a period when help is needed at home.
Second, review the coverage gaps that matter most for aging well. Medicare choices, prescription coverage, Medigap or Medicare Advantage tradeoffs, dental and vision needs, and long-term services and supports can all affect both cash flow and independence. This is not a one-time decision; plans, premiums, formularies, networks, and health needs can change.
Third, protect the behaviors that protect healthspan. If cost pressure leads someone to skip medication, delay care, avoid preventive visits, or ignore mobility and home-safety needs, the financial issue can become a health issue. A Wealthspan plan should leave room for the boring but powerful basics: medication access, primary care, strength and fall-prevention work, food, transportation, and a safe home environment.
Fourth, track the trend, not just the headline. One year of higher costs may be manageable. A pattern of rising premiums, higher drug spending, growing credit card balances, or shrinking emergency savings deserves attention sooner rather than later.
A simple annual checkup for health-care affordability
Once a year, write down five numbers: monthly health insurance premiums, average monthly prescription costs, expected out-of-pocket medical costs, emergency savings, and retirement savings contributions or withdrawals. Then ask one question: if health costs rose again next year, what would bend first?
That question is not meant to create anxiety. It is meant to reveal fragility while there is still time to adjust. For some households, the next step may be comparing Medicare options during open enrollment. For others, it may be rebuilding emergency savings, checking eligibility for assistance programs, reviewing HSA strategy before Medicare, updating a retirement income plan, or discussing lower-cost medication options with a clinician or pharmacist.
Because Wealthspan is about preserving independence and quality of life, the goal is not simply to spend less on care. The goal is to avoid being forced into worse choices later because the cost of care was never made visible in the plan.
The bottom line
This week’s most important Wealthspan development is not one market headline. It is the reminder that health-care affordability is becoming a central retirement resilience issue for older adults.
AARP’s new survey shows broad financial strain among adults 50 and older. KFF’s Medicare brief shows that coverage does not eliminate affordability pressure after age 65. Together, they point to a practical conclusion: a serious aging plan should include a health-care cost plan.
That does not mean predicting every future bill. It means making medical costs visible, reviewing coverage regularly, protecting savings from avoidable shocks, and treating health-care affordability as part of the foundation for independence.
Keep Building Your Wealthspan
Start with Wealth Span 101 for the core financial habits that support long-term wellbeing.
Estimate future medical costs with the Retirement Healthcare Spend Estimator.
Model savings decisions with the Retirement Savings Calculator.
Track both money and health trends in the Annual Wealthspan + Healthspan Checkup Tracker.
-
AARP. “Older Americans Feeling Financial Strain as Costs Rise, New AARP Report Finds.” Published May 28, 2026. https://www.aarp.org/press/releases/2026-05-28-older-americans-feeling-financial-strain-as-costs-rise/
AARP Research. “AARP Financial Security Trends Survey, January 2026.” Published May 2026. DOI: 10.26419/res.01076.001. https://www.aarp.org/pri/topics/work-finances-retirement/financial-security-retirement/financial-security-trends-survey-wave7/
KFF. “Key Facts About Health Care Affordability for People With Medicare.” Published May 27, 2026. https://www.kff.org/medicare/key-facts-about-health-care-affordability-for-people-with-medicare/
Employee Benefit Research Institute. “New EBRI Report Finds Some Medicare Households May Need Nearly $500,000 for Health Care in Retirement.” Published March 11, 2026. https://www.ebri.org/content/new-ebri-report-finds-some-medicare-households-may-need-nearly--500-000-for-health-care-in-retirement
Centers for Medicare & Medicaid Services. “NHE Fact Sheet.” Accessed May 28, 2026. https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/nhe-fact-sheet
Ng, A. E., Adjaye-Gbewonyo, D., & Ward, B. W. “Prescription Medication Use and Cost-Related Nonadherence Among Adults Age 65 and Older in the United States, 2021–2022.” National Health Statistics Reports, No. 209. Published September 5, 2024. https://www.cdc.gov/nchs/data/nhsr/nhsr209.pdf
Han, X., Zhao, J., Zheng, Z., de Moor, J. S., Virgo, K. S., Yabroff, K. R. “Medical Financial Hardship Intensity and Financial Sacrifice Associated with Cancer in the United States.” Cancer Epidemiology, Biomarkers & Prevention, 29(2), 308-317. 2020. DOI: 10.1158/1055-9965.EPI-19-0460. https://doi.org/10.1158/1055-9965.EPI-19-0460