
Lifestyle Is a Healthspan Lever
A new 21-year JAMA follow-up of the Diabetes Prevention Program suggests intensive lifestyle change may help delay the pileup of chronic conditions in adults who started with prediabetes.
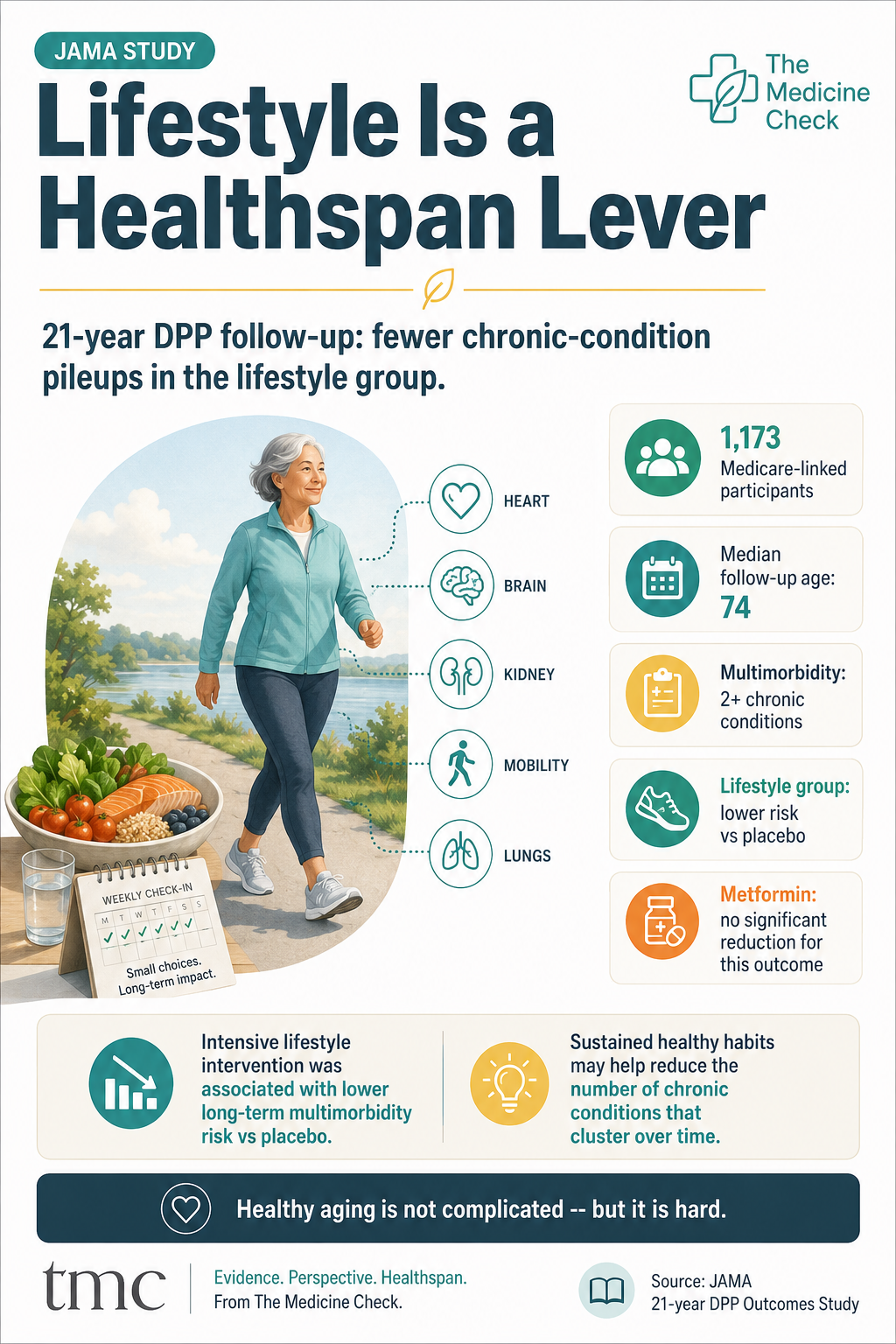
Infographic explaining that a 21-year Diabetes Prevention Program follow-up linked intensive lifestyle intervention with lower long-term multimorbidity risk in adults with prediabetes.
The healthspan question is not just how long you live. It is how many conditions pile up along the way.
Most longevity headlines chase one disease, one drug, one supplement, or one biomarker. But real healthspan is often shaped by something less glamorous: whether chronic conditions accumulate slowly enough that a person can preserve function, independence, cognition, mobility, and quality of life.
That is why a new JAMA study published online June 15, 2026, is worth paying attention to. Researchers looked back at adults who entered the landmark Diabetes Prevention Program with prediabetes in the late 1990s, then followed Medicare-linked outcomes through 2021. The question was not only whether lifestyle change or metformin delayed diabetes. It was whether either intervention was associated with less long-term multimorbidity, meaning two or more chronic conditions.
The headline finding was practical and healthspan-centered: participants originally assigned to intensive lifestyle intervention had a lower risk of multimorbidity over 21 years of follow-up compared with placebo. The metformin group did not show a statistically significant reduction in this particular outcome compared with placebo.
What the study actually tested
The analysis drew from the Diabetes Prevention Program and its long-term follow-up, the Diabetes Prevention Program Outcomes Study. The original trial enrolled 3,234 adults at high risk for diabetes from 1996 to 1999 at 27 U.S. sites. Participants were randomly assigned to one of three groups: intensive lifestyle intervention, metformin, or placebo.
For this new multimorbidity analysis, the researchers used Centers for Medicare & Medicaid Services claims data for 1,173 consenting participants who had Medicare-linked information available through 2021. Their median age by the end of follow-up was 74 years.
The lifestyle program was not a vague instruction to “be healthier.” During the original trial, it included 16 individual sessions, followed by ongoing support. The goals were reduced calories and fat, at least 150 minutes of physical activity per week, and weight loss of at least 7% from baseline. Later, all participants were offered group lifestyle sessions, and the original lifestyle group received additional booster sessions for years.
The main finding
By the end of follow-up, multimorbidity was common in all three groups. That matters. Lifestyle change did not erase chronic disease risk, and the study should not be read as a promise that diet and exercise prevent aging.
Still, the differences were meaningful. In the JAMA report, 82% of participants in the lifestyle group, 85% in the metformin group, and 87% in the placebo group experienced two or more chronic conditions. After adjustment for relevant factors, the lifestyle group had a lower risk of multimorbidity compared with placebo. The hazard ratio was 0.79, with a 95% confidence interval of 0.68 to 0.93. Metformin was not significantly different from placebo for this outcome.
NIH summarized the practical result this way: compared with placebo, the lifestyle group had a 21% lower risk for two chronic conditions and a 25% lower risk for three chronic conditions. The association also persisted when diabetes was removed from the multimorbidity definition, suggesting the signal was not only a diabetes-counting artifact.
When researchers looked at dyads of the costliest conditions, the lifestyle association was even stronger. JAMA reported a hazard ratio of 0.57 for lifestyle versus placebo for those high-cost combinations.
Why this matters for healthspan
Aging well is not simply avoiding one diagnosis. It is avoiding the compounding effect of many diagnoses at once.
One chronic condition can often be managed. Two, three, or five conditions can begin to interact. Medications multiply. Specialist visits increase. Fatigue, pain, glucose control, sleep disruption, kidney function, cardiovascular risk, depression, mobility limitations, and fall risk can reinforce one another. That pileup is what often narrows a person’s day-to-day options.
This is why multimorbidity is such a useful healthspan outcome. It gets closer to the real question readers care about: not “Can I optimize a lab marker?” but “Can I preserve the capacity to keep living the way I want to live?”
The new JAMA study supports a grounded message: for adults at high risk of diabetes, sustained lifestyle support may have benefits that extend beyond delaying diabetes alone. It may also reduce the long-term burden of clustered chronic conditions.
What this does not prove
This analysis focused on adults who started with prediabetes or high diabetes risk. It should not be treated as proof that the same effect size applies to everyone.
The multimorbidity outcomes were based on Medicare claims data. Claims are useful for long-term follow-up, but they are not the same as direct clinical exams of every condition.
The lifestyle intervention was intensive and supported. The result should not be simplified into “just try harder.” Program design, coaching, access, food environment, safety, time, and social support all matter.
The metformin finding is outcome-specific. Metformin remains an important medication for type 2 diabetes care and diabetes prevention in selected high-risk patients. This study does not mean metformin has no value.
Multimorbidity still occurred in most participants. The finding is about lower risk and delayed burden, not complete prevention.
The practical takeaway
The most useful lesson is not that lifestyle is magic. It is that lifestyle is infrastructure.
For healthspan, the basics are not basic because they are easy. They are basic because they support multiple systems at once: glucose regulation, blood pressure, vascular health, muscle, mobility, sleep, mood, inflammation, kidney risk, and cardiovascular resilience.
A reasonable annual Healthspan check-in does not need to become a perfection project. It can start with a few measurable questions:
Am I getting regular movement, including enough walking or aerobic activity to support metabolic and cardiovascular health?
Am I doing some form of strength training or resistance work to protect muscle and mobility?
Do I know my key metabolic markers, including A1C or fasting glucose when appropriate, blood pressure, cholesterol, weight trend, and waist trend?
Am I eating in a way that makes healthier choices repeatable, not heroic?
Do I have support, accountability, or a program structure that makes behavior change easier to sustain?
For readers who want a structured place to review both health and planning markers, The Medicine Check Annual Wealthspan + Healthspan Checkup Tracker is a useful next step: https://www.themedicinecheck.com/annual-wealthspan-healthspan-checkup-tracker
The bottom line
This week’s strongest Healthspan development is not a flashy anti-aging claim. It is a long follow-up from a serious prevention trial showing that intensive lifestyle intervention was associated with a lower long-term burden of chronic-condition clustering among adults who began with prediabetes.
That is a durable healthspan message. The goal is not to chase the newest longevity promise. The goal is to keep fewer diseases from stacking up, protect function, and preserve more room for independence over time.
Keep Building Your Healthspan
Track your yearly progress with the Annual Wealthspan + Healthspan Checkup Tracker.
If medications are part of the story, review your list with the Anticholinergic Burden Calculator.
-
Salive ME, Tjaden AH, Ames JR, et al. Lifestyle and Metformin Interventions and Risk of Multimorbidity in Adults With Prediabetes. JAMA. Published online June 15, 2026. doi:10.1001/jama.2026.8492. https://jamanetwork.com/journals/jama/article-abstract/2850450
National Institutes of Health. For adults with prediabetes, lifestyle intervention lowered risk of developing multiple chronic conditions. Published June 15, 2026. https://www.nih.gov/news-events/news-releases/adults-prediabetes-lifestyle-intervention-lowered-risk-developing-multiple-chronic-conditions
Florez H, Foster C, Vizcaino G. Addressing Multimorbidity Challenges in Diabetes--Lifestyle and Beyond. JAMA. Published online June 15, 2026. doi:10.1001/jama.2026.10080. https://jamanetwork.com/journals/jama/article-abstract/2850456
The Diabetes Prevention Program Research Group. The Diabetes Prevention Program: design and methods for a clinical trial in the prevention of type 2 diabetes. Diabetes Care. 1999;22(4):623-634. doi:10.2337/diacare.22.4.623.